Maxillomandibular Advancement (MMA) | Orthognathic Surgery
Bite, Breathing & Beauty
The name says advancement.
Riley and Powell built maxillomandibular advancement around breathing. Over the past decade I have planned it for two more things at the same time: the bite it leaves behind, and the balance of the face. The jaws are not simply moved forward. They are rotated about a fixed center so all three improve together.
Bite
The upper and lower jaws move as one unit into a planned bite, so your teeth still meet correctly after surgery. In many cases this can be done surgery-first, which shortens the time spent in braces.
The maxillomandibular complex is rotated counterclockwise about a center at the maxillary buttress, keeping the first-molar level and preserving the designed occlusion. Surgery-first sequencing is practical when orthodontic leveling is limited.
Breathing
Advancing and rotating the jaws carries the tongue and palate forward and, just as important, restores tension to the airway muscles so the airway holds open during sleep.
Beyond enlarging the airway, MMA stabilizes the lateral pharyngeal wall and reverses concentric velar collapse on DISE. Airflow modeling shows reduced retropalatal velocity and downstream negative pressure, which track with AHI and ODI improvement.
Beauty
The jaws frame the lower face, so moving them in balance tends to strengthen the profile and chin. The changes to the face and nose are planned in advance, not left to chance.
The center of rotation is chosen to allow mandibular advancement without a protrusive midface, while septoplasty, turbinate reduction, piriformplasty, and an alar cinch manage the nose. Patient-reported nasal function and cosmesis improve with this approach.
Dr. Liu’s Select Chapters on MMA and Skeletal Sleep Surgery
How does maxillomandibular advancement work?
For years the benefit of jaw advancement was attributed to making more room behind the tongue. Our work showed the more important change happens at the soft palate and side walls of the throat. Using drug-induced sleep endoscopy before and after surgery, we found that the largest measurable effect of maxillomandibular advancement is a reduction in collapse of the velum and lateral pharyngeal walls.
A follow-up study using computational fluid dynamics confirmed it: the patients whose apnea improved the most were the ones whose lateral wall stability and airflow had normalized. This is one reason maxillomandibular advancement can help patients whose soft palate collapses in a complete concentric pattern, the same pattern that rules out hypoglossal nerve stimulation on its own.
As for the tongue, post-operative myofunctional therapy can be very helpful. For patients who still need more support, the combination of maxillomandibular advancement and hypoglossal nerve stimulation has shown reliability in treating sleep apnea. They work in complementary ways.
Virtual Surgical Planning
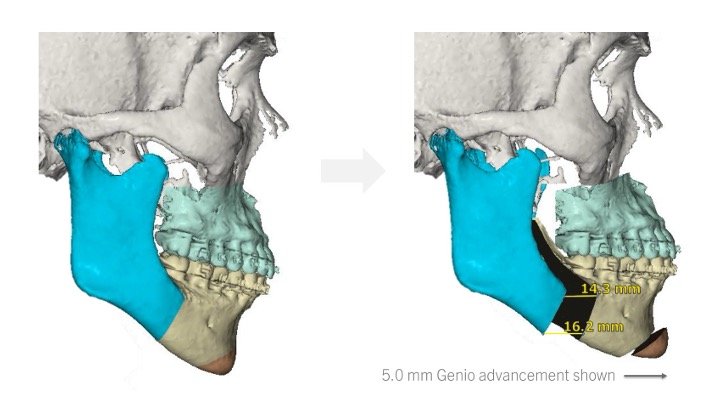
Typical counterclockwise rotation for a high angle, class 2 patient
Maxillary cant, yaw, midline correction | Rotation center decision for CCR
Advancement at the piriform rim Advancement at pogonion