Septoplasty (Video for Patients)
Septoplasty — For Referring Physicians
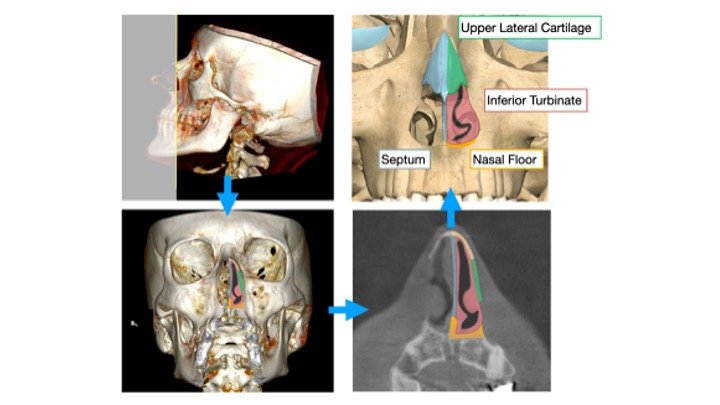
The internal nasal valve (INV) is comprised of the septum, inferior turbinates, caudal edge of the upper lateral cartilages, and the bony nasal floor. The INV can account for up to 50% of total upper airway resistance. In patients with sleep-disordered breathing, even modest nasal obstruction increases the negative inspiratory pressure that promotes pharyngeal collapse during sleep.
Septoplasty addresses deviations of the quadrangular cartilage, vomer, and maxillary crest components that contribute to INV narrowing. Critical septal support structures, particularly the dorsal and caudal L-strut, are preserved to maintain nasal integrity.
In our practice, septoplasty is frequently performed in conjunction with inferior turbinate reduction (radiofrequency ablation with outfracture) and, when indicated, nasal valve repair or piriformplasty. For patients with transverse maxillary hypoplasia contributing to a narrow nasal floor, distraction osteogenesis maxillary expansion (DOME) offers an adjunctive approach to widen the INV at its skeletal foundation.
Correction of nasal obstruction has been shown to improve sleep quality and enhance adherence to positive airway pressure therapy. It also serves as a foundational intervention within the updated Stanford Sleep Surgery Algorithm, which integrates site-directed nasal, palatal, tongue base, neurostimulation, and skeletal procedures based on individual patient phenotyping.
Septoplasty — For Patients
The nasal septum is the wall of cartilage and bone that divides the nose into two passages. When it is crooked or shifted to one side — a "deviated septum" — it can block airflow through one or both nostrils.
Many people notice this during the day, but the effect on breathing is often worse during sleep. When the nose is obstructed, the body works harder to pull air through a narrower space, which can contribute to snoring and sleep apnea.
Septoplasty straightens the deviated portions of the septum to improve airflow. The procedure is performed entirely through the nostrils. There are no external incisions and no change to the appearance of the nose.
I often combine septoplasty with reduction of the inferior turbinates (the tissue ridges inside the nose) to achieve the best result. For patients whose narrow palate contributes to nasal obstruction, maxillary expansion (DOME) may also be discussed.
The goal is to restore comfortable nasal breathing — especially during sleep.
Components of the Internal Nasal Valve